Dental Medical Clearance Form
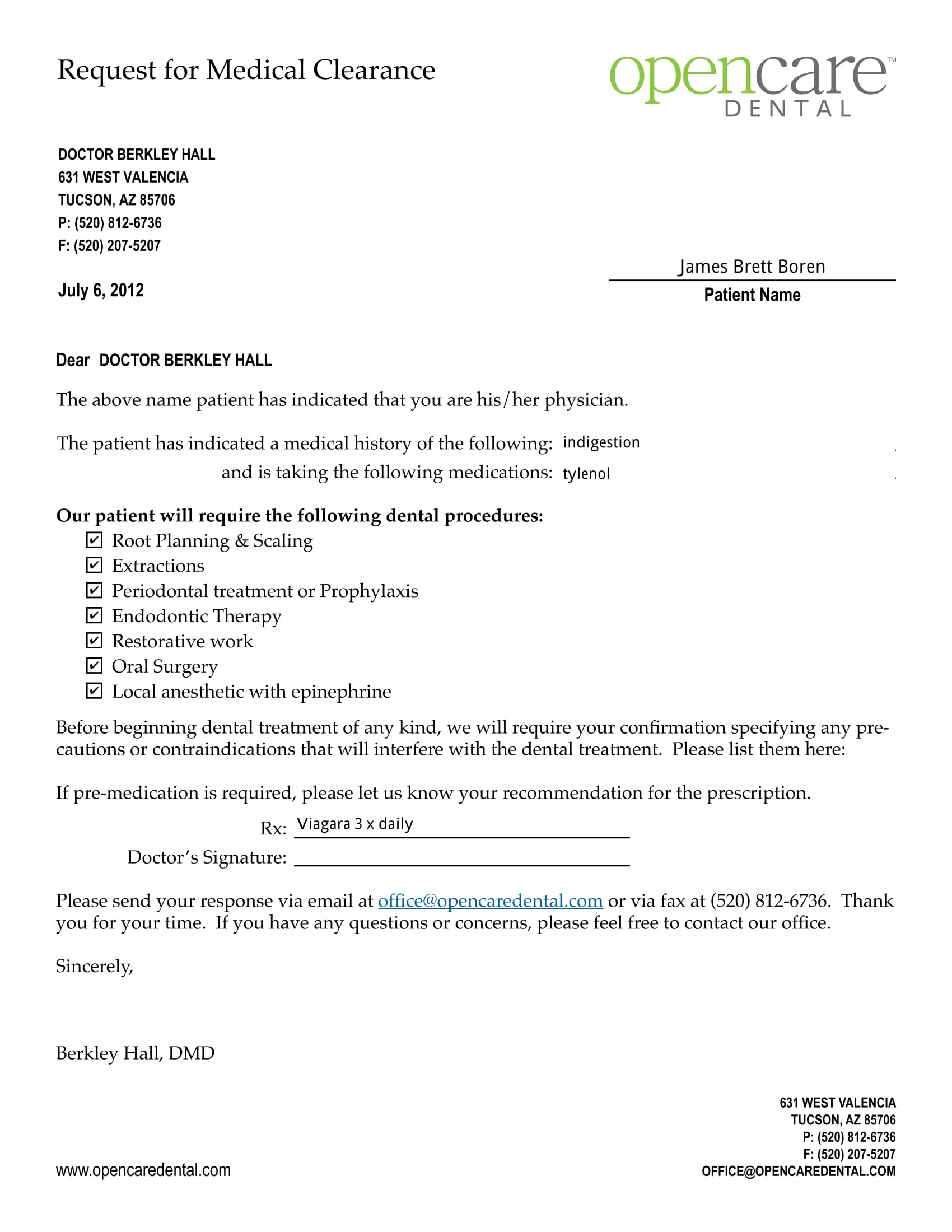
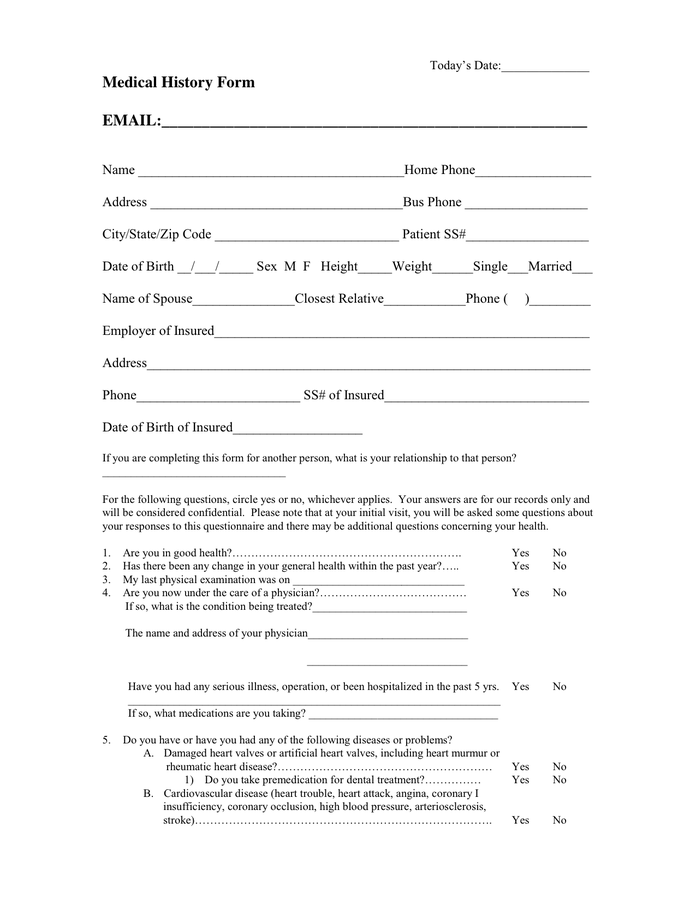
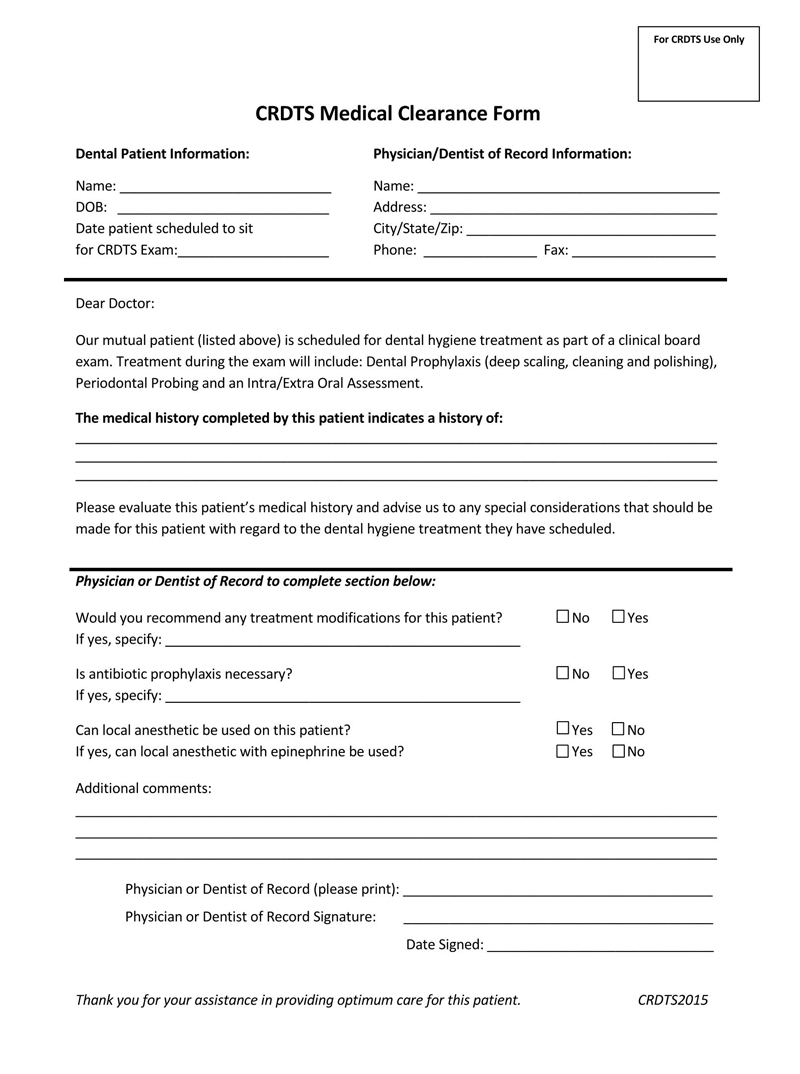
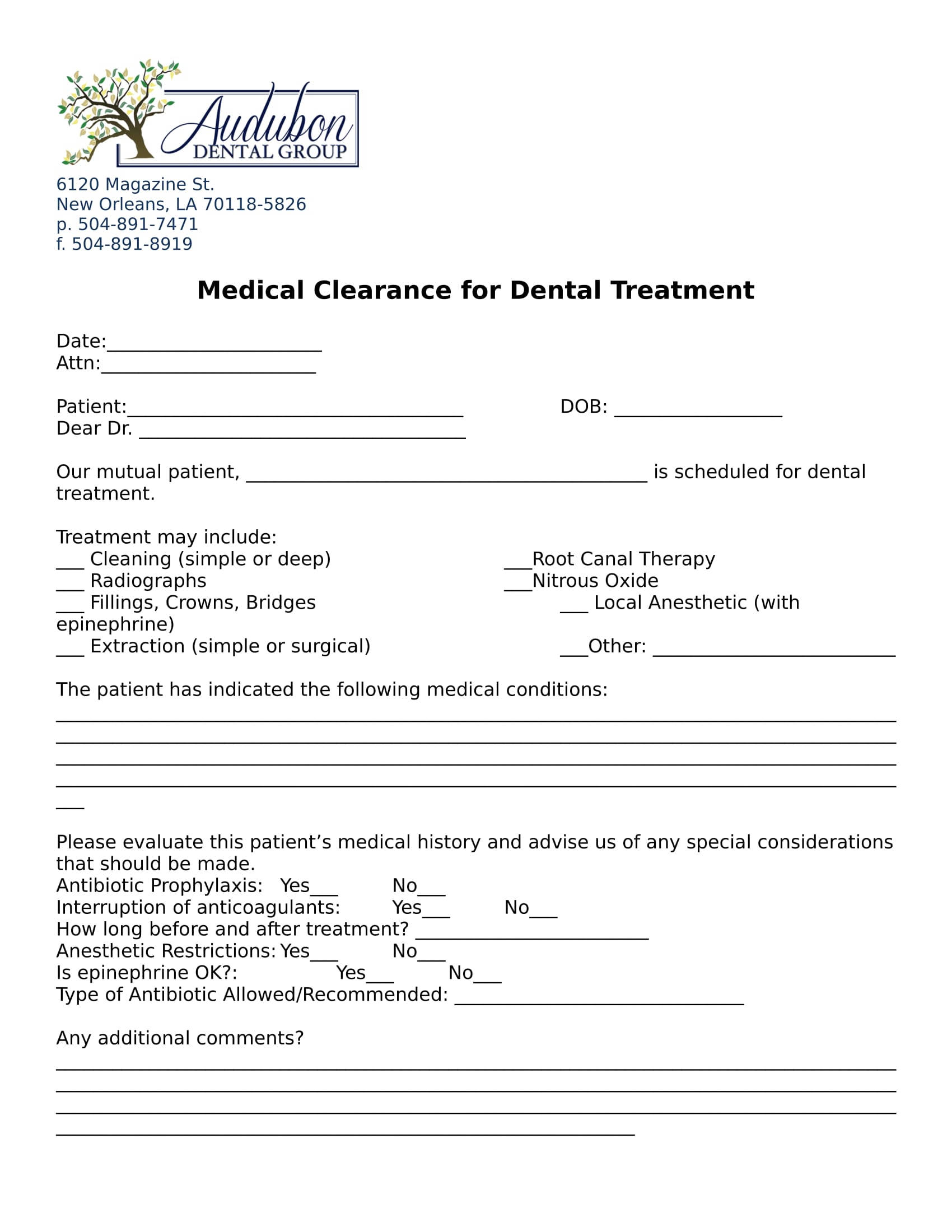
Dental Medical Clearance Form - Our mutual patient has presented for dental treatment with the following medical problem(s): The following treatment is scheduled in our dental. Medical clearance for dental surgery dear _____, m.d.: Our mutual patient, _____, is planning on having dental surgery with local. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure.
Our mutual patient has presented for dental treatment with the following medical problem(s): Medical clearance for dental surgery dear _____, m.d.: The following treatment is scheduled in our dental. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Our mutual patient, _____, is planning on having dental surgery with local.
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Our mutual patient has presented for dental treatment with the following medical problem(s): Our mutual patient, _____, is planning on having dental surgery with local. Medical clearance for dental surgery dear _____, m.d.: The following treatment is scheduled in our dental.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Our mutual patient has presented for dental treatment with the following medical problem(s): Medical clearance for dental surgery dear _____, m.d.: Our mutual patient, _____, is planning on having dental surgery with local. The following treatment is scheduled in our dental. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance for dental surgery dear _____, m.d.: The following treatment is scheduled in our dental. Our mutual patient, _____, is planning on having dental surgery with local. Our mutual patient has presented for dental treatment with the following.
FREE 31+ Medical Clearance Forms in PDF MS Word
The following treatment is scheduled in our dental. Our mutual patient has presented for dental treatment with the following medical problem(s): Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Our mutual patient, _____, is planning on having dental surgery with local. Medical clearance for dental surgery dear.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Medical clearance for dental surgery dear _____, m.d.: Our mutual patient, _____, is planning on having dental surgery with local. Our mutual patient has presented for dental treatment with the following medical problem(s): The following treatment is scheduled in our dental. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Our mutual patient, _____, is planning on having dental surgery with local. Our mutual patient has presented for dental treatment with the following medical problem(s): Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance for dental surgery dear _____, m.d.: The following treatment is scheduled in.
Medical Clearance Form For Dental Treatment templates free printable
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Our mutual patient, _____, is planning on having dental surgery with local. Medical clearance for dental surgery dear _____, m.d.: Our mutual patient has presented for dental treatment with the following medical problem(s): The following treatment is scheduled in.
Printable For Dental Medical Clearance Form
Medical clearance for dental surgery dear _____, m.d.: The following treatment is scheduled in our dental. Our mutual patient, _____, is planning on having dental surgery with local. Our mutual patient has presented for dental treatment with the following medical problem(s): Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Our mutual patient, _____, is planning on having dental surgery with local. Medical clearance for dental surgery dear _____, m.d.: Our mutual patient has presented for dental treatment with the following medical problem(s): Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. The following treatment is scheduled in.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Our mutual patient has presented for dental treatment with the following medical problem(s): Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. The following treatment is scheduled in our dental. Medical clearance for dental surgery dear _____, m.d.: Our mutual patient, _____, is planning on having dental surgery.

Printable Medical Clearance Form For Surgery
Our mutual patient has presented for dental treatment with the following medical problem(s): The following treatment is scheduled in our dental. Our mutual patient, _____, is planning on having dental surgery with local. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance for dental surgery dear.
Our Mutual Patient Has Presented For Dental Treatment With The Following Medical Problem(S):
Our mutual patient, _____, is planning on having dental surgery with local. The following treatment is scheduled in our dental. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance for dental surgery dear _____, m.d.: