Formexpress Scripts Appeal Form
Formexpress Scripts Appeal Form - Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; You may also ask us for an appeal. Prescription drug coverage this application for second level appeal should be used to. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Medicare clinical appeals po box 66588 st. Express scripts application for second level appeal:
If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Medicare clinical appeals po box 66588 st. You may also ask us for an appeal. Express scripts application for second level appeal: Prescription drug coverage this application for second level appeal should be used to. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and;
You may also ask us for an appeal. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Express scripts application for second level appeal: Prescription drug coverage this application for second level appeal should be used to. Medicare clinical appeals po box 66588 st. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision.
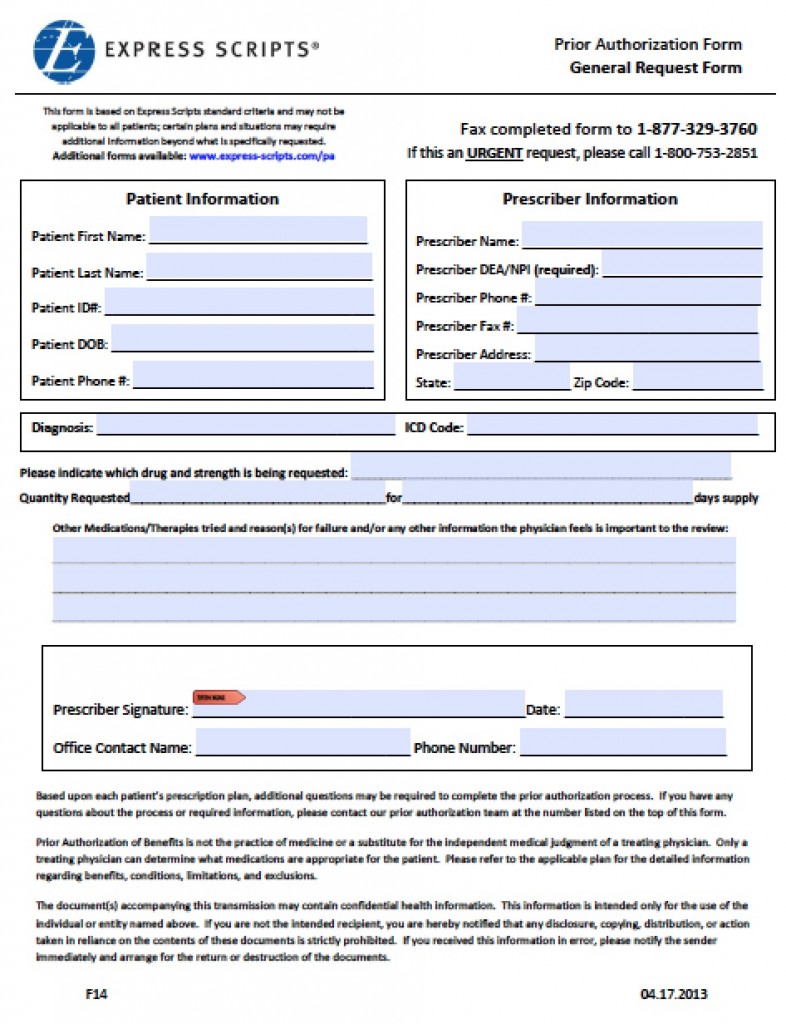
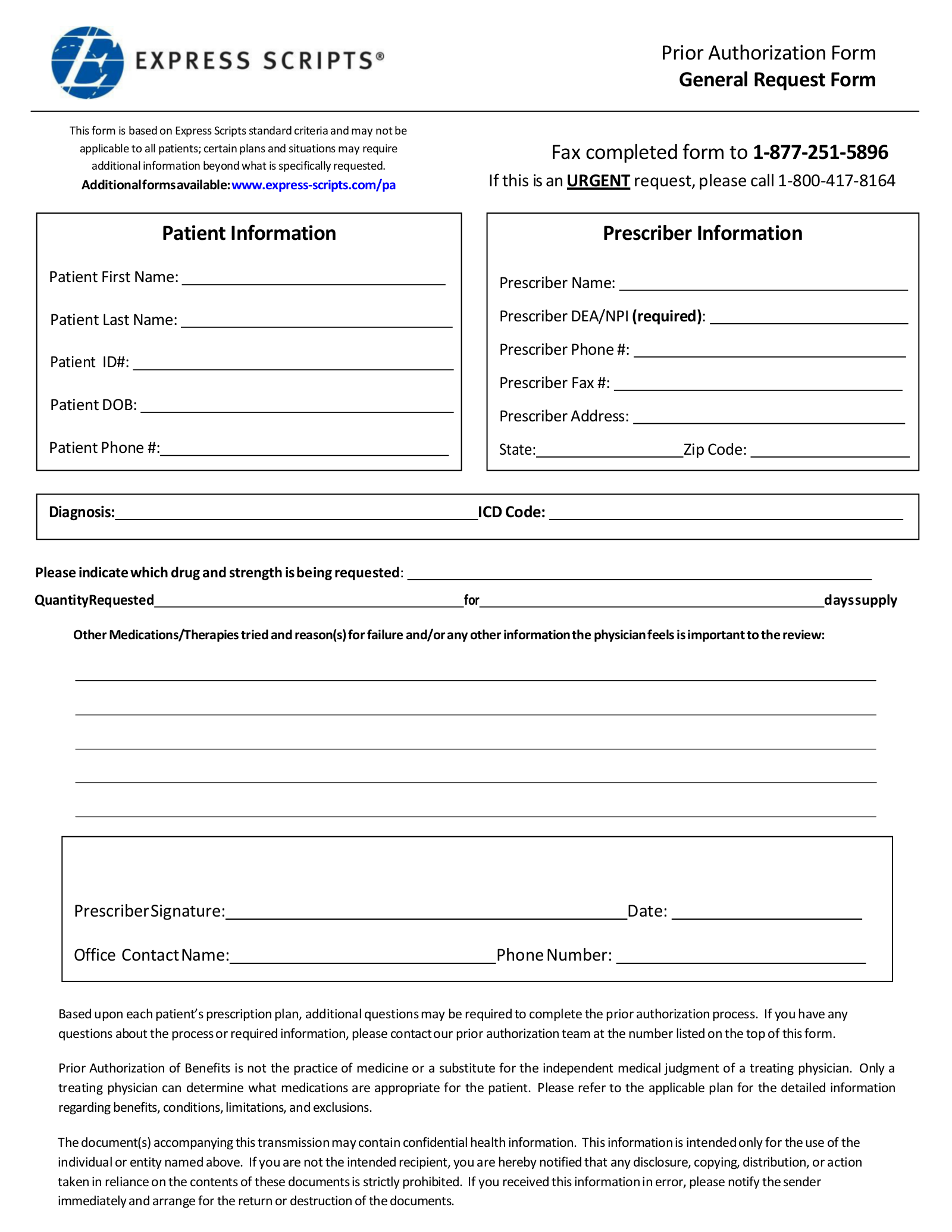
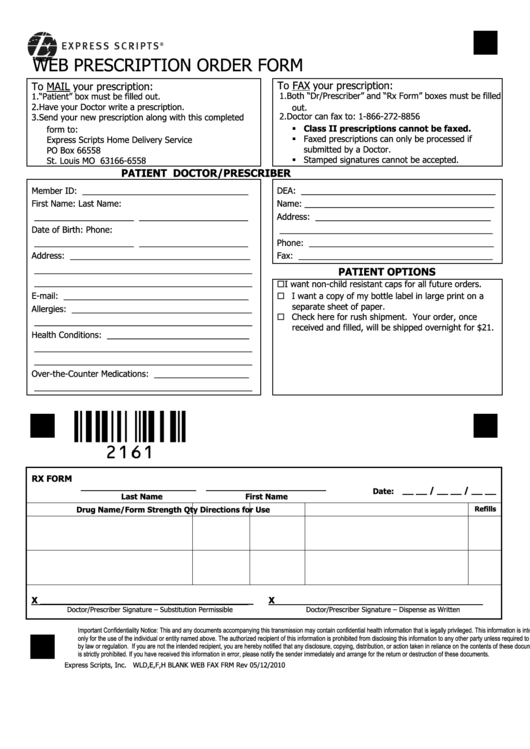
Download Express Scripts Prior Authorization Fax Form PDF wikiDownload
You may also ask us for an appeal. Prescription drug coverage this application for second level appeal should be used to. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Medicare clinical appeals po box 66588 st. Express scripts application for second level appeal:
Express Scripts Tier Exception Form 2023 Printable Forms Free Online
You may also ask us for an appeal. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Medicare clinical appeals po box 66588 st. Express scripts application for second level appeal: Prescription drug coverage this application for second level appeal should be used to.
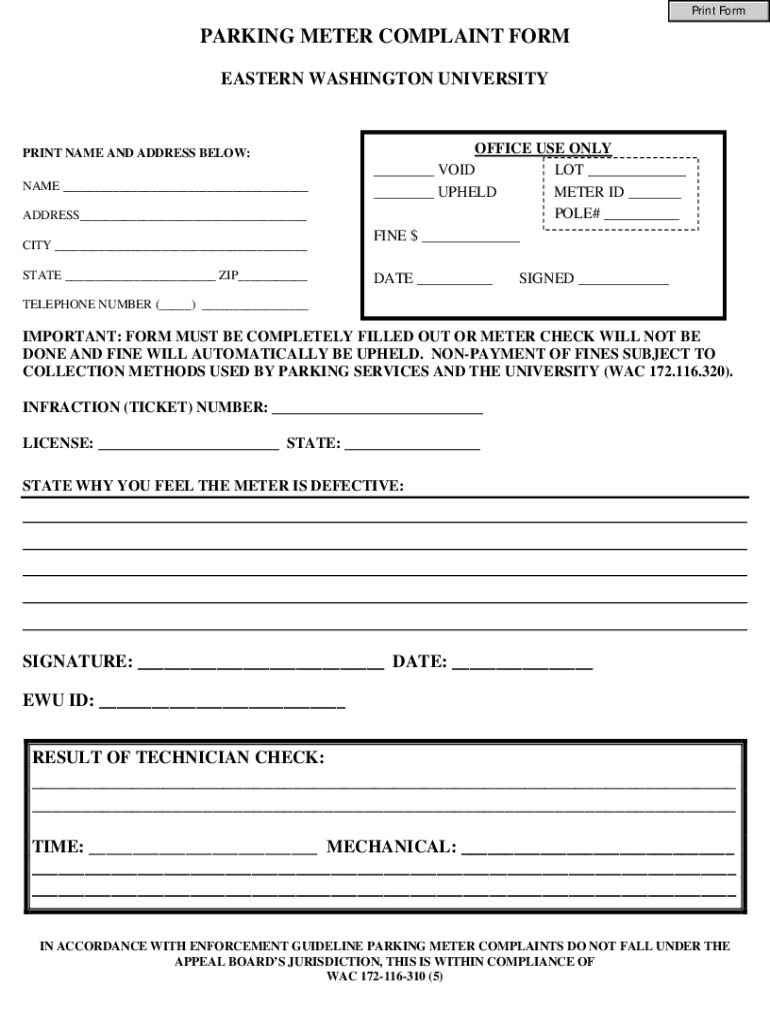
Fillable Online Appeal FormMeter Fax Email Print pdfFiller
Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Prescription drug coverage this application for second level appeal should be used to. You may also ask us for an appeal. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision..
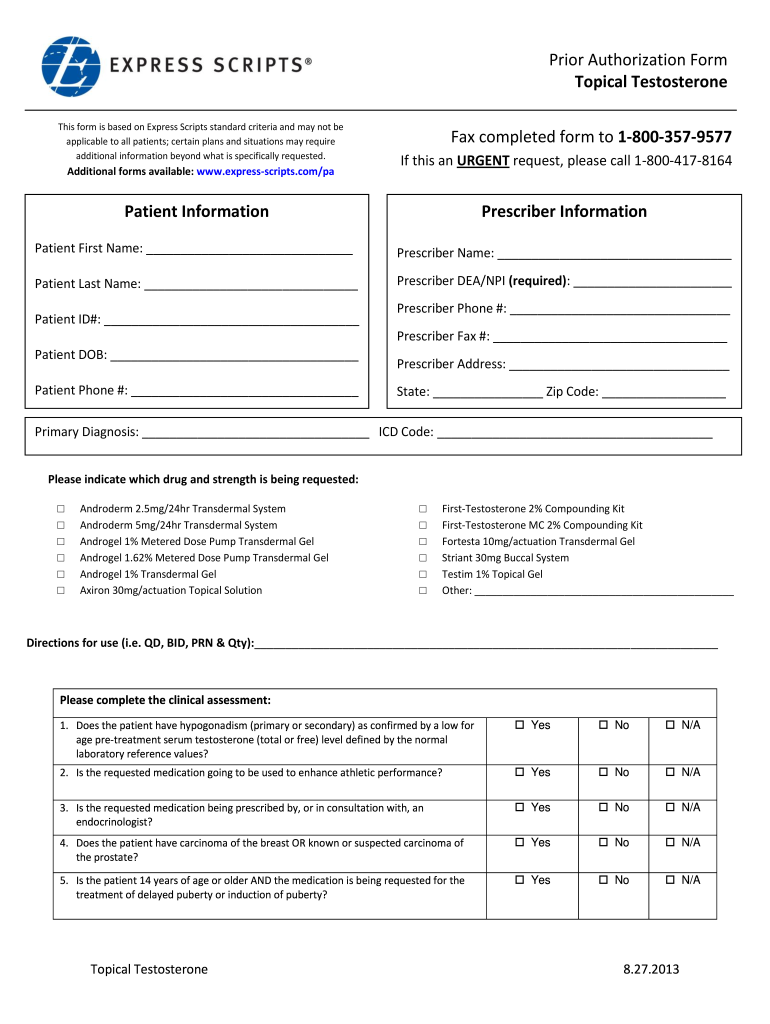
Express Scripts Prior Authorization 20132024 Form Fill Out and Sign
If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Medicare clinical appeals po box 66588 st. Express scripts application for second level appeal: Prescription drug coverage this application for second.

Express scripts appeal form Fill out & sign online DocHub
Express scripts application for second level appeal: Prescription drug coverage this application for second level appeal should be used to. You may also ask us for an appeal. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; If your request for prescription coverage was denied, you have the right to ask.

Fillable Online Express Scripts Review And Appeals Form. Express
Express scripts application for second level appeal: Prescription drug coverage this application for second level appeal should be used to. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; You.
Top 16 Express Scripts Forms And Templates free to download in PDF format
Express scripts application for second level appeal: If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Medicare clinical appeals po box 66588 st. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; You may also ask us for an.

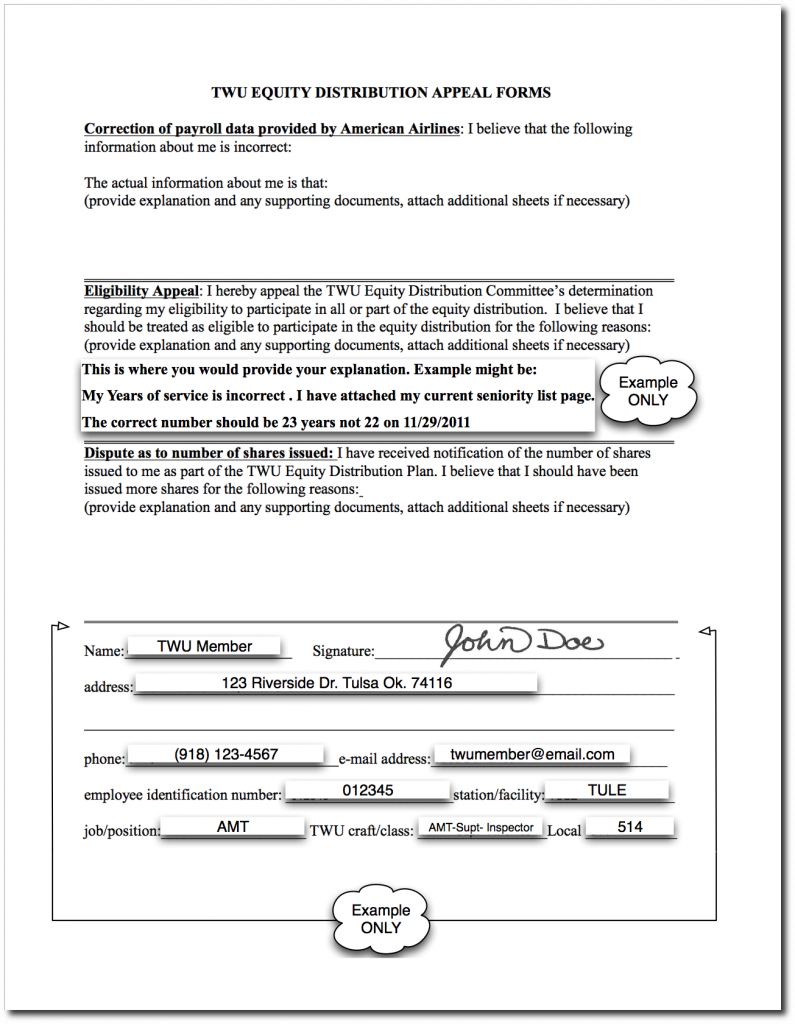
FM BHS SUPT Appeal Form Arabic PDF
Prescription drug coverage this application for second level appeal should be used to. You may also ask us for an appeal. Medicare clinical appeals po box 66588 st. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; If your request for prescription coverage was denied, you have the right to ask.
57 HQ Images Express Scripts Appeal Form Express Scripts Prior
Prescription drug coverage this application for second level appeal should be used to. Express scripts application for second level appeal: Medicare clinical appeals po box 66588 st. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. You may also ask us for an appeal.
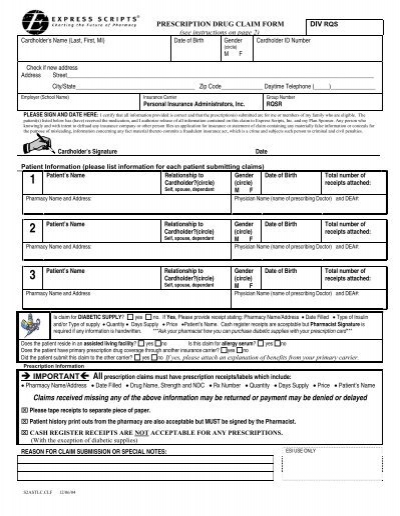
Claim Form for Express Scripts Prescriptions
Express scripts application for second level appeal: Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Medicare clinical appeals po box 66588 st. You may also ask us for an appeal. If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our.
You May Also Ask Us For An Appeal.
If your request for prescription coverage was denied, you have the right to ask for a redetermination (appeal) of our decision. Medicare clinical appeals po box 66588 st. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Prescription drug coverage this application for second level appeal should be used to.