Formhipaa Acknowledgement Form
Formhipaa Acknowledgement Form - Hipaa acknowledgement and consent form i understand that under the health insurance portability and accountability act of 1996. Patient hipaa acknowledgment and consent form _____ (patient initials) notice of privacy practices. ________ (patient/representative initials) i acknowledge that i have received the notice of privacy practice, which describes the ways in. This hipaa patient acknowledgment form outlines the consent and authorization necessary for processing health information. I acknowledge that i have received the. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health.
Hipaa acknowledgement and consent form i understand that under the health insurance portability and accountability act of 1996. Patient hipaa acknowledgment and consent form _____ (patient initials) notice of privacy practices. ________ (patient/representative initials) i acknowledge that i have received the notice of privacy practice, which describes the ways in. I acknowledge that i have received the. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. This hipaa patient acknowledgment form outlines the consent and authorization necessary for processing health information. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health.
Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health. Hipaa acknowledgement and consent form i understand that under the health insurance portability and accountability act of 1996. Patient hipaa acknowledgment and consent form _____ (patient initials) notice of privacy practices. I acknowledge that i have received the. This hipaa patient acknowledgment form outlines the consent and authorization necessary for processing health information. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. ________ (patient/representative initials) i acknowledge that i have received the notice of privacy practice, which describes the ways in.

Acknowledgement Form PDF
Patient hipaa acknowledgment and consent form _____ (patient initials) notice of privacy practices. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. Hipaa acknowledgement and consent form i understand.

Nys Fillable Employee Policy Acknowledgement Form Printable Forms The
Patient hipaa acknowledgment and consent form _____ (patient initials) notice of privacy practices. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health. This hipaa patient acknowledgment form outlines the consent and authorization necessary for processing health information. This file is a hipaa omnibus rule, patient acknowledgement form.

Acknowledgement Form PDF
________ (patient/representative initials) i acknowledge that i have received the notice of privacy practice, which describes the ways in. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health. Hipaa acknowledgement and consent form i understand that under the health insurance portability and accountability act of 1996. This.
Acknowledgement in Research Forms Docs 2023
I acknowledge that i have received the. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. Hipaa acknowledgement and consent form i understand that under the health insurance portability and accountability act of 1996. ________ (patient/representative initials) i acknowledge that i have received the notice of privacy practice, which describes the.

Fillable Online Free Medical Records Release Authorization FormHIPAA
I acknowledge that i have received the. ________ (patient/representative initials) i acknowledge that i have received the notice of privacy practice, which describes the ways in. Hipaa acknowledgement and consent form i understand that under the health insurance portability and accountability act of 1996. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy.
Generic Acknowledgement Form, Generic Acknowledgement Form Template
I acknowledge that i have received the. This hipaa patient acknowledgment form outlines the consent and authorization necessary for processing health information. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. Hipaa acknowledgement and consent form i understand that under the health insurance portability and accountability act of 1996. Hipaa acknowledgement.
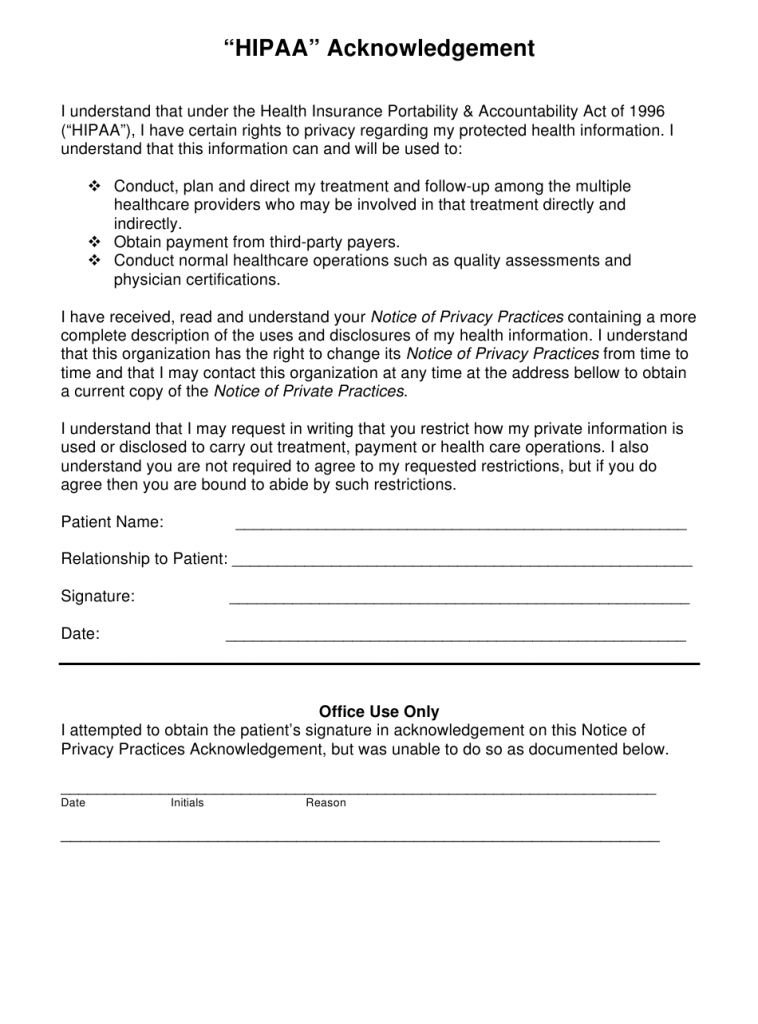
Acknowledgement Form For Hipaa
This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. This hipaa patient acknowledgment form outlines the consent and authorization necessary for processing health information. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health. I acknowledge that i have.
Partnership Notary Acknowledgement Form, Notary Acknowledgement Form
________ (patient/representative initials) i acknowledge that i have received the notice of privacy practice, which describes the ways in. This hipaa patient acknowledgment form outlines the consent and authorization necessary for processing health information. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. Hipaa acknowledgement and consent form i understand that.
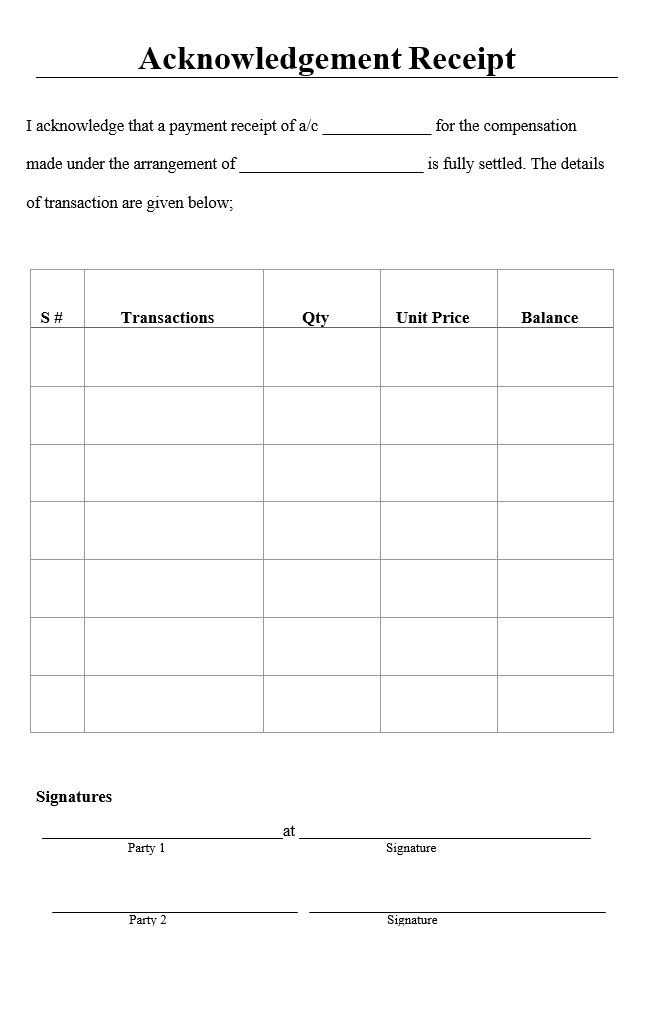
Acknowledgement Receipt Sample PDF Free Word & Excel Templates
This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health. ________ (patient/representative initials) i acknowledge that i have received the notice of privacy practice, which describes the ways in. I.
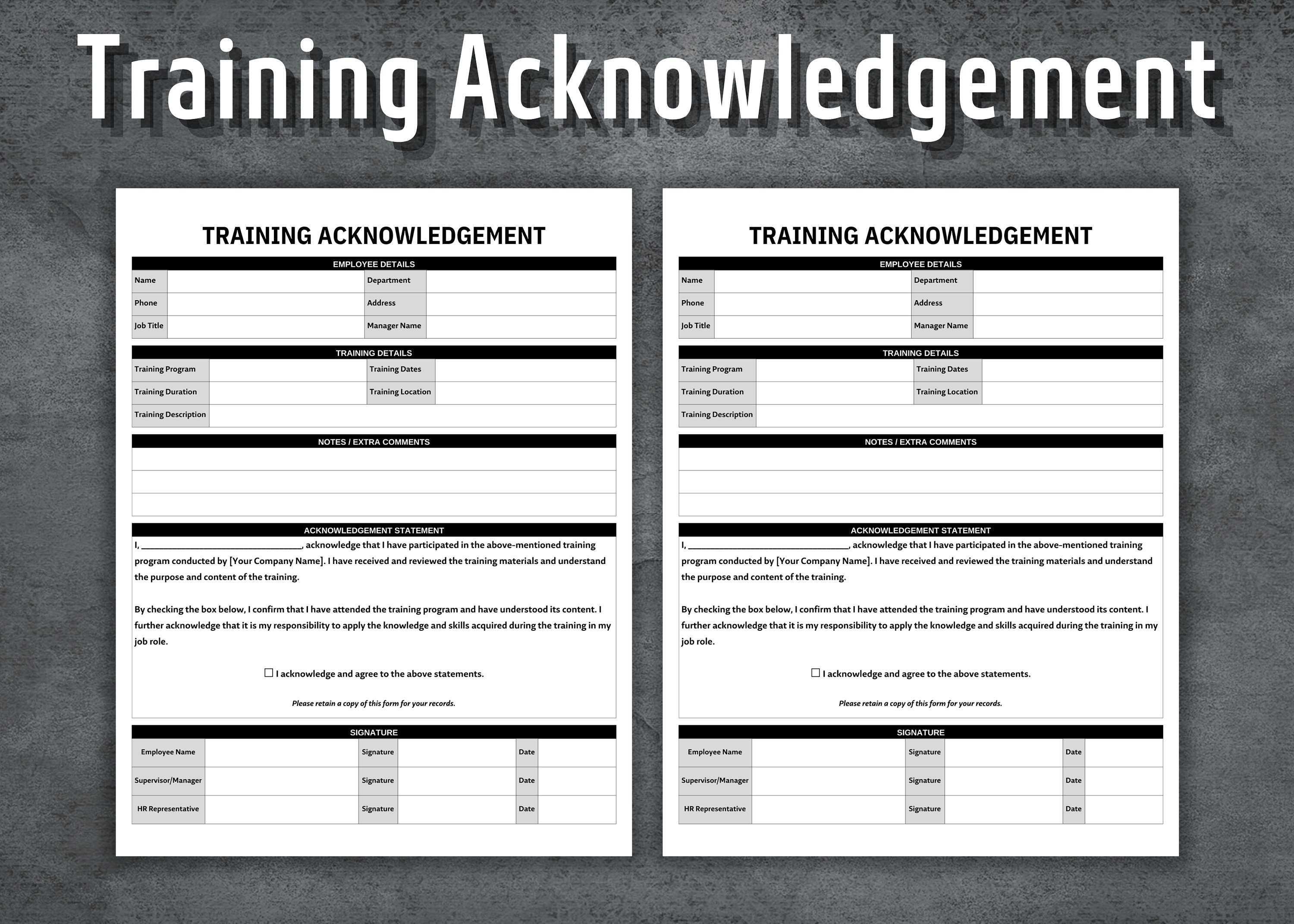
Training Acknowledgement Form, Printable Training Templates, HR
This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited. I acknowledge that i have received the. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health. ________ (patient/representative initials) i acknowledge that i have received the notice of privacy.
________ (Patient/Representative Initials) I Acknowledge That I Have Received The Notice Of Privacy Practice, Which Describes The Ways In.
I acknowledge that i have received the. Hipaa acknowledgement & release form notice of privacy practices print name of patient _____ date of birth _____ we, at atlantic health. Hipaa acknowledgement and consent form i understand that under the health insurance portability and accountability act of 1996. This file is a hipaa omnibus rule, patient acknowledgement form for receipt of notice of privacy practices, consent/limited.
This Hipaa Patient Acknowledgment Form Outlines The Consent And Authorization Necessary For Processing Health Information.
Patient hipaa acknowledgment and consent form _____ (patient initials) notice of privacy practices.