Kaiser Permanente Appeal Form
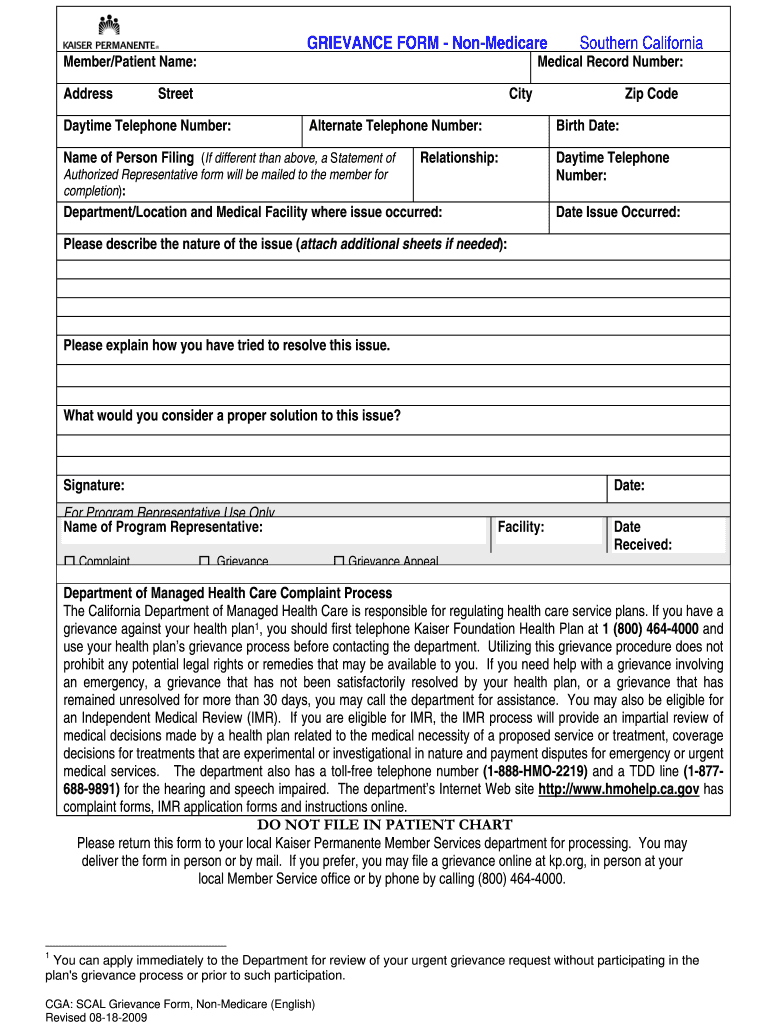
Kaiser Permanente Appeal Form - Reason for denial, member name & date of birth, medical record number, service dates and. Attach denial documents and other records or documents that support your request. Appeals criteria and time frames for resolution are identical for. Looking for information about the services we offer? Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Appeal is submitted without appeal filing form, the information listed below must be present: View, download, or print commonly used forms, guidebooks, handbooks, and other publications. If you believe that kaiser health plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance. You must make your request to kaiser permanente orally or in writing before the member receives the services in question.
Appeal is submitted without appeal filing form, the information listed below must be present: View, download, or print commonly used forms, guidebooks, handbooks, and other publications. You must make your request to kaiser permanente orally or in writing before the member receives the services in question. Appeals criteria and time frames for resolution are identical for. Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Attach denial documents and other records or documents that support your request. If you believe that kaiser health plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance. Reason for denial, member name & date of birth, medical record number, service dates and. Looking for information about the services we offer?
Attach denial documents and other records or documents that support your request. Appeal is submitted without appeal filing form, the information listed below must be present: If you believe that kaiser health plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance. Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Appeals criteria and time frames for resolution are identical for. View, download, or print commonly used forms, guidebooks, handbooks, and other publications. Looking for information about the services we offer? You must make your request to kaiser permanente orally or in writing before the member receives the services in question. Reason for denial, member name & date of birth, medical record number, service dates and.

The Kaiser PermanenteGeisinger deal Questions and answers
You must make your request to kaiser permanente orally or in writing before the member receives the services in question. Looking for information about the services we offer? Appeal is submitted without appeal filing form, the information listed below must be present: Reason for denial, member name & date of birth, medical record number, service dates and. If you believe.

kaiser permanente appeal form Yanira Braswell
Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. If you believe that kaiser health plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance. View, download, or print commonly used forms, guidebooks, handbooks, and.
kaiser permanente appeal form Yanira Braswell
You must make your request to kaiser permanente orally or in writing before the member receives the services in question. Reason for denial, member name & date of birth, medical record number, service dates and. Attach denial documents and other records or documents that support your request. Appeals criteria and time frames for resolution are identical for. View, download, or.

Kaiser Permanente MidAtlantic Health Plans Achieve Top Quality Ratings
You must make your request to kaiser permanente orally or in writing before the member receives the services in question. Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. If you believe that kaiser health plan has failed to provide these services or discriminated in another way on the basis of race, color, national.
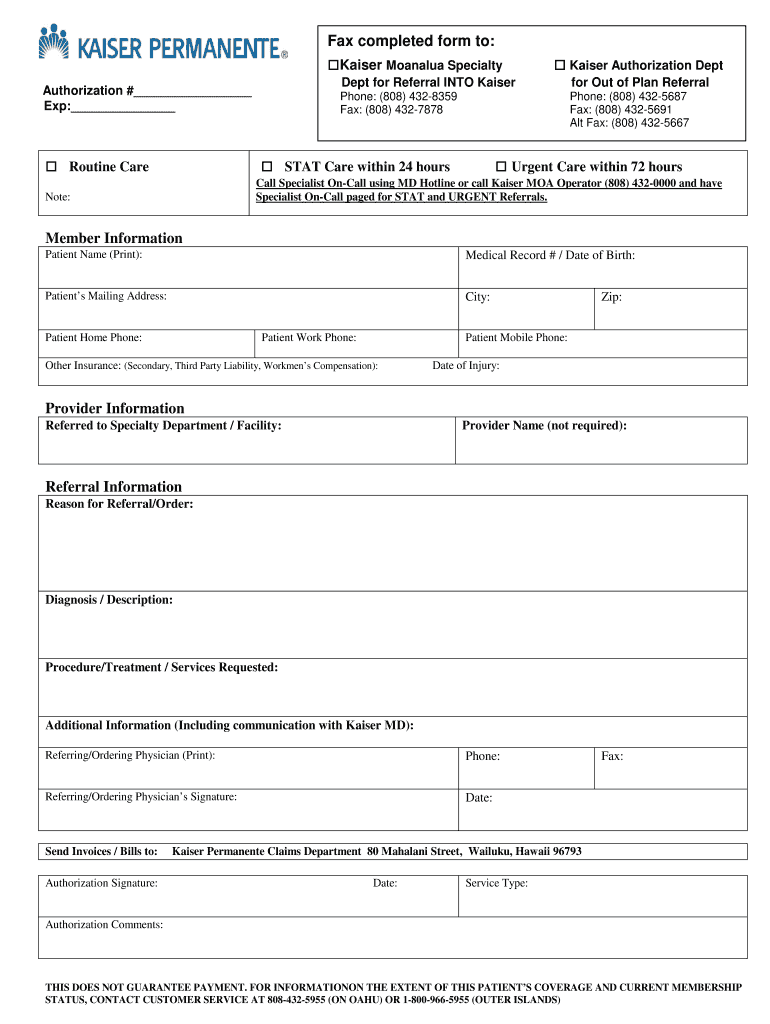
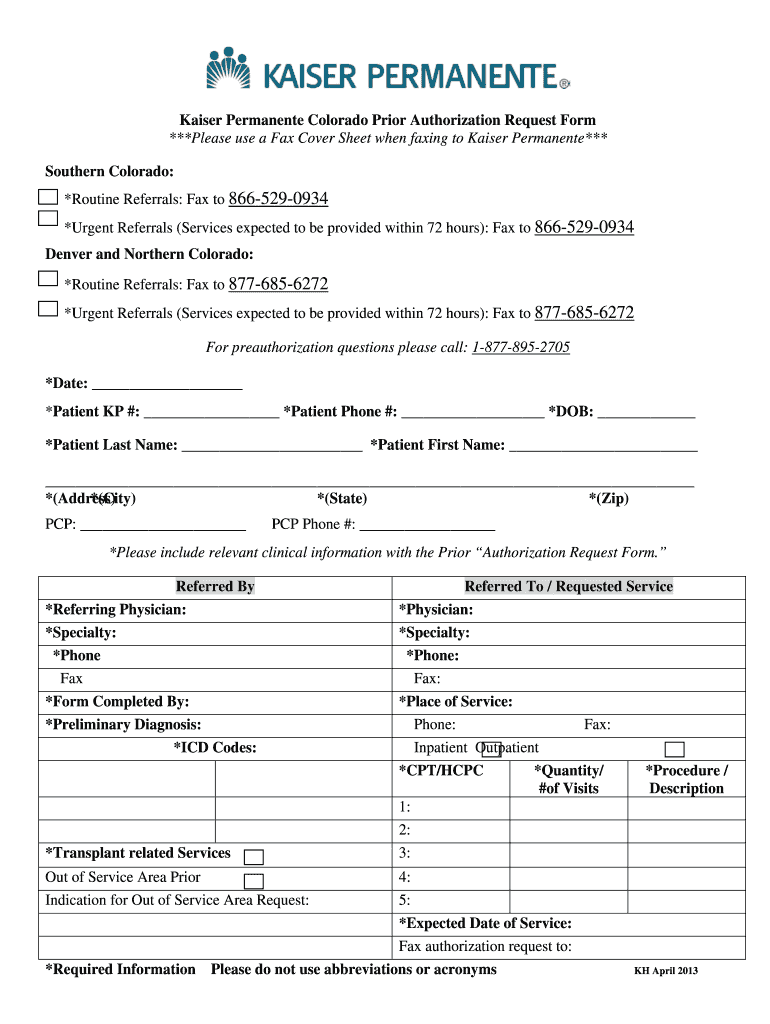
Kaiser Permanente Authorization Form
Reason for denial, member name & date of birth, medical record number, service dates and. You must make your request to kaiser permanente orally or in writing before the member receives the services in question. Looking for information about the services we offer? Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Appeal is.

How Health Insurers Can Appeal to Millennials
Reason for denial, member name & date of birth, medical record number, service dates and. Looking for information about the services we offer? Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Attach denial documents and other records or documents that support your request. Appeals criteria and time frames for resolution are identical for.
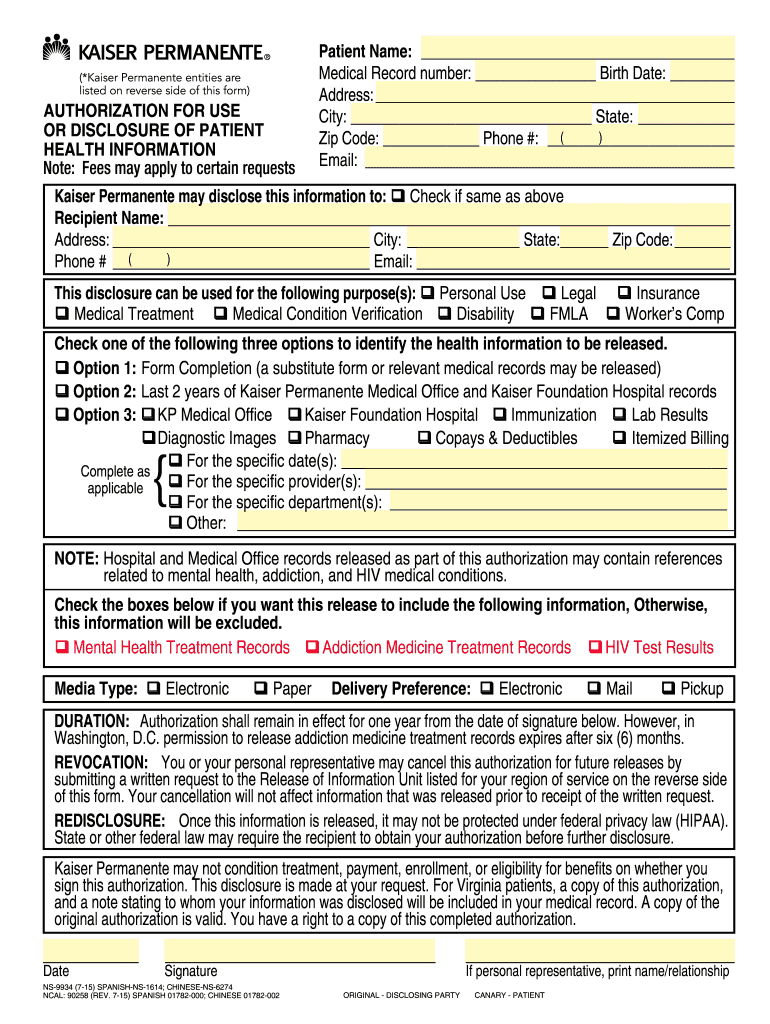
Kaiser Roi Form Tiba Abidi
Attach denial documents and other records or documents that support your request. Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Appeal is submitted without appeal filing form, the information listed below must be present: If you believe that kaiser health plan has failed to provide these services or discriminated in another way on.
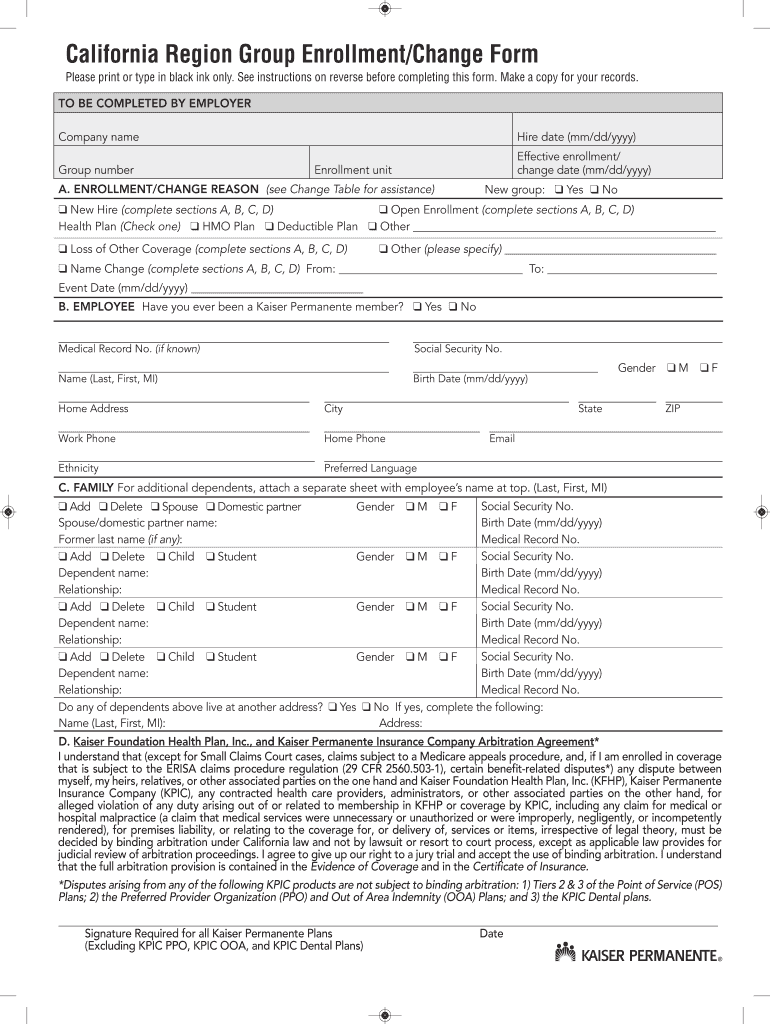
CA Kaiser Permanente Region Group Enrollment/Change Form 2011 Fill
Attach denial documents and other records or documents that support your request. You must make your request to kaiser permanente orally or in writing before the member receives the services in question. Appeals criteria and time frames for resolution are identical for. Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Appeal is submitted.
kaiser permanente appeal form Yanira Braswell
Appeals criteria and time frames for resolution are identical for. Appeal is submitted without appeal filing form, the information listed below must be present: Looking for information about the services we offer? Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Attach denial documents and other records or documents that support your request.
Colorado Kaiser Permanente 20132024 Form Fill Out and Sign Printable
Looking for information about the services we offer? Health care and/or financial dependent power of attorney form stipulating you are currently authorized to. Reason for denial, member name & date of birth, medical record number, service dates and. You must make your request to kaiser permanente orally or in writing before the member receives the services in question. Appeals criteria.
You Must Make Your Request To Kaiser Permanente Orally Or In Writing Before The Member Receives The Services In Question.
Looking for information about the services we offer? View, download, or print commonly used forms, guidebooks, handbooks, and other publications. If you believe that kaiser health plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance. Appeals criteria and time frames for resolution are identical for.
Health Care And/Or Financial Dependent Power Of Attorney Form Stipulating You Are Currently Authorized To.
Appeal is submitted without appeal filing form, the information listed below must be present: Attach denial documents and other records or documents that support your request. Reason for denial, member name & date of birth, medical record number, service dates and.