Medicaid Hysterectomy Consent Form
Medicaid Hysterectomy Consent Form - The name must match the name on the. Patient name must be complete and legible (full first and last name, no initials). _____ date of hysterectomy procedure: Hysterectomy acknowledgement form revised 12/01/2015. Division of budget and analysis. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. Please give to the north carolina disaster relief fund to help communities recover from helene.
_____ date of hysterectomy procedure: Patient name must be complete and legible (full first and last name, no initials). 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. The name must match the name on the. Division of budget and analysis. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials. Hysterectomy acknowledgement form revised 12/01/2015. Please give to the north carolina disaster relief fund to help communities recover from helene.
Division of budget and analysis. Patient name must be complete and legible (full first and last name, no initials). The name must match the name on the. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. Hysterectomy acknowledgement form revised 12/01/2015. _____ date of hysterectomy procedure: Please give to the north carolina disaster relief fund to help communities recover from helene. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials.

Ohio Medicaid Hysterectomy Consent Form 2024
11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. Please give to the north carolina disaster relief fund to help communities recover from helene. Hysterectomy acknowledgement form revised 12/01/2015. Division of budget and analysis. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials.
Fillable Online Nc Medicaid Hysterectomy Consent Form. Nc Medicaid
_____ date of hysterectomy procedure: Please give to the north carolina disaster relief fund to help communities recover from helene. Hysterectomy acknowledgement form revised 12/01/2015. The name must match the name on the. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,.

Hysterectomy Consent Form For Ohio Medicaid 2023 Printable Consent
Patient name must be complete and legible (full first and last name, no initials). The name must match the name on the. _____ date of hysterectomy procedure: Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,.

Medicaid Hysterectomy Consent Form Texas 2024 Printable Consent Form 2024
Please give to the north carolina disaster relief fund to help communities recover from helene. _____ date of hysterectomy procedure: 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. Division of budget and analysis. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials.
Texas Disclosure and Consent for Hysterectomy Fill Out, Sign Online
11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. Division of budget and analysis. _____ date of hysterectomy procedure: Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials. Please give to the north carolina disaster relief fund to help communities recover from helene.

Hysterectomy consent form Fill out & sign online DocHub
Hysterectomy acknowledgement form revised 12/01/2015. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. _____ date of hysterectomy procedure: Division of budget and analysis. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials.

Ohio Medicaid Hysterectomy Consent Form 2023 Printable Consent Form 2022
_____ date of hysterectomy procedure: Patient name must be complete and legible (full first and last name, no initials). The name must match the name on the. Please give to the north carolina disaster relief fund to help communities recover from helene. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,.

Mississippi Medicaid Consent Form 2022 Printable Consent Form 2022
Patient name must be complete and legible (full first and last name, no initials). The name must match the name on the. Please give to the north carolina disaster relief fund to help communities recover from helene. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials. Division of budget and analysis.

Medicaid Hysterectomy Consent Form North Carolina 2024 Printable
Hysterectomy acknowledgement form revised 12/01/2015. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. The name must match the name on the. Division of budget and analysis. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials.

Pennsylvania Medicaid Sterilization Consent Form 2022 Printable
Please give to the north carolina disaster relief fund to help communities recover from helene. The name must match the name on the. Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials. Hysterectomy acknowledgement form revised 12/01/2015. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic.
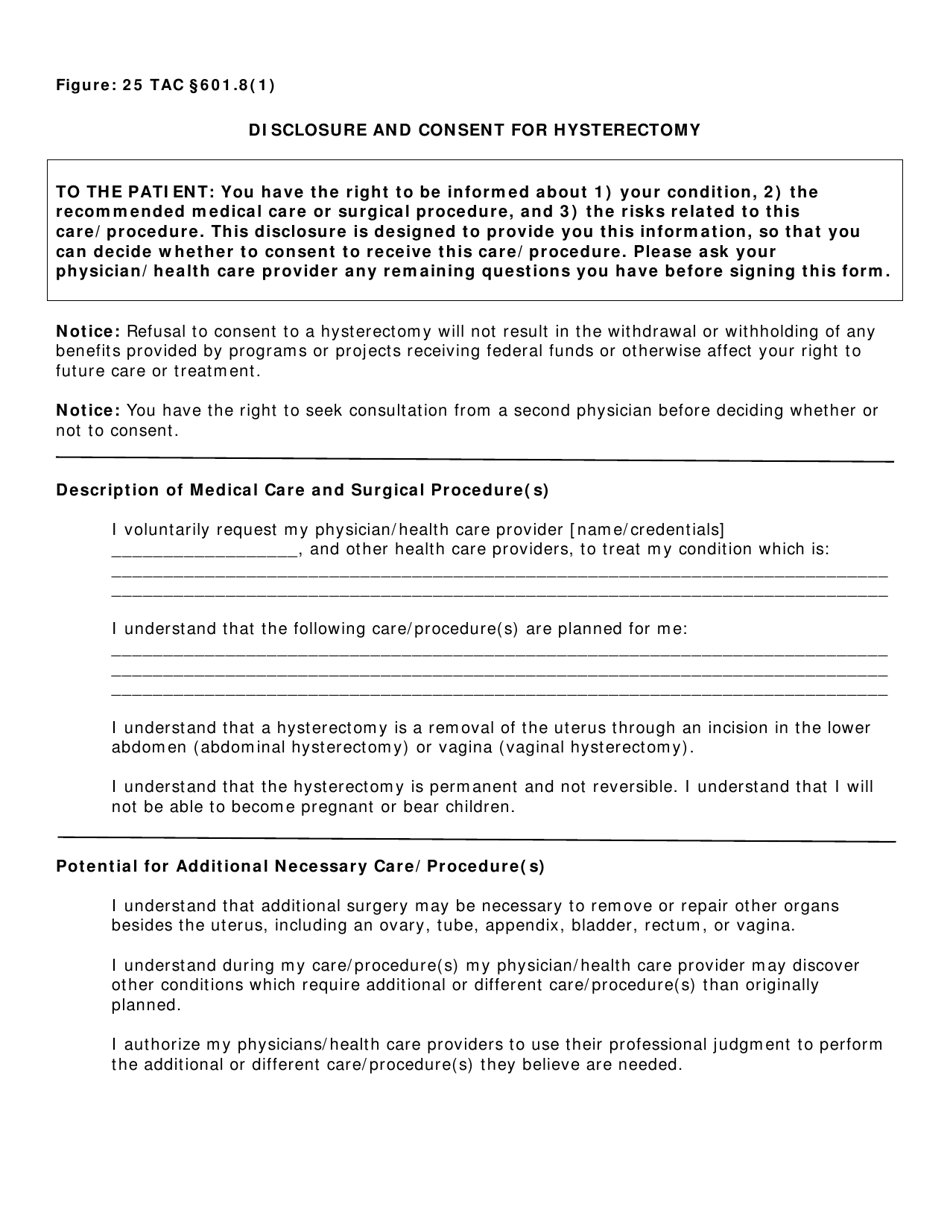
Patient Name Must Be Complete And Legible (Full First And Last Name, No Initials).
Please give to the north carolina disaster relief fund to help communities recover from helene. 11 rows medicaid forms required by the north carolina departments of social services dental and orthodontic dental/orthodontic services,. _____ date of hysterectomy procedure: Some providers of ob/gyn services have been receiving sterilization consent form and hysterectomy statement denials.
Hysterectomy Acknowledgement Form Revised 12/01/2015.
Division of budget and analysis. The name must match the name on the.