The Written Medical Dental Health History Form
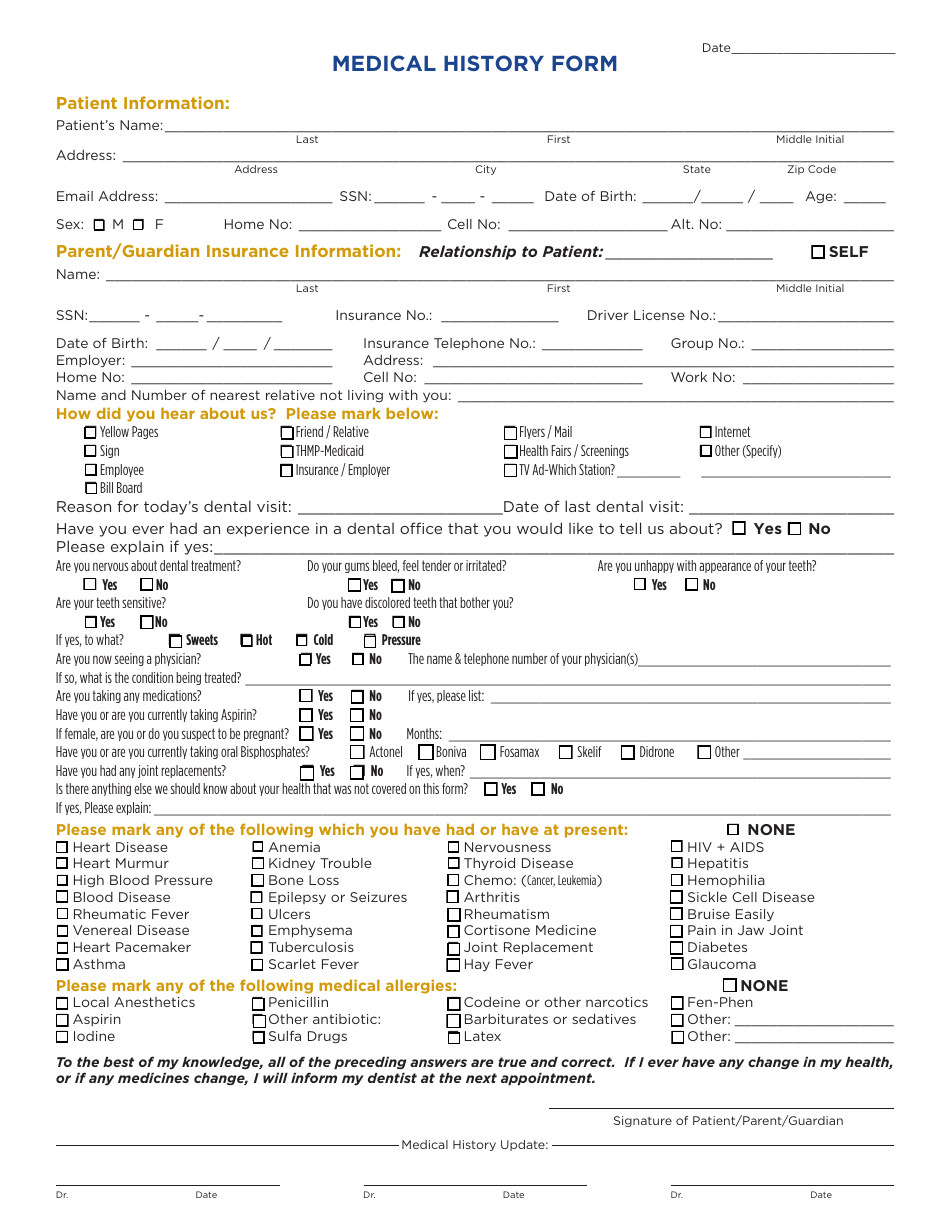
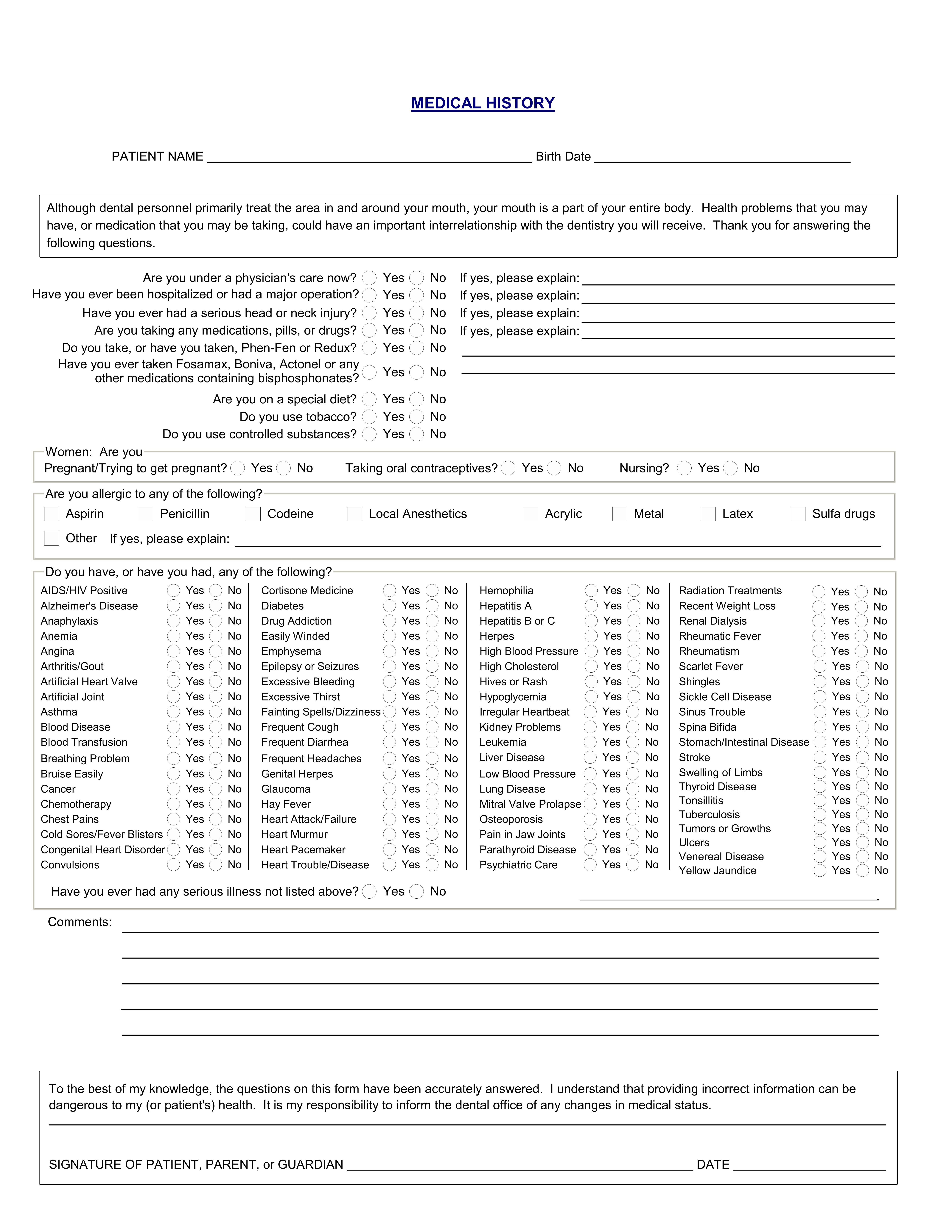
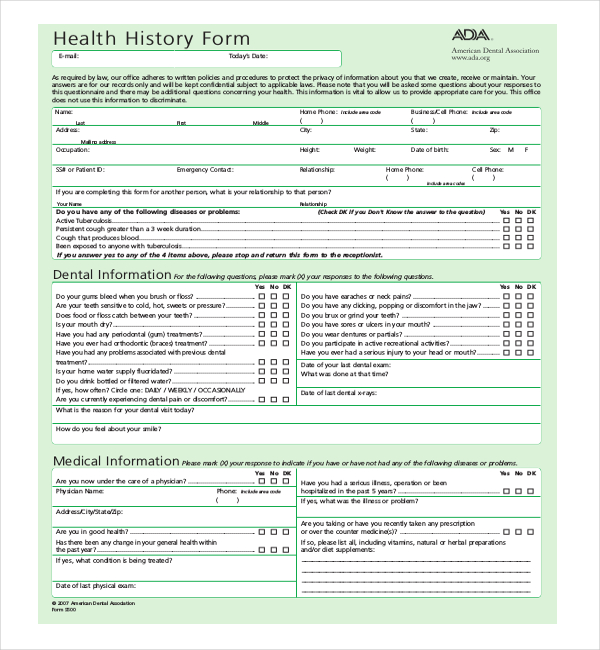
The Written Medical Dental Health History Form - Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical conditions they might have,. Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. Both doctor and patient are encouraged to. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online.
Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. Both doctor and patient are encouraged to. Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical conditions they might have,. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues.
Both doctor and patient are encouraged to. Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical conditions they might have,. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues.

Printable Medical History Form For Dental Office Printable Word Searches
Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. Use the 2021 edition of the ada patient dental and medical health history information.

Printable Medical History Form For Dental Office Printable Forms Free
The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. Medical information please mark (x) your response to indicate if.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-03-scaled-e1617709269345.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
Both doctor and patient are encouraged to. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. Sample health history.
Printable Dental Medical History Form Template Printable Templates
Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. Both doctor and patient are encouraged to. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. This form provides a detailed overview of.
.png)
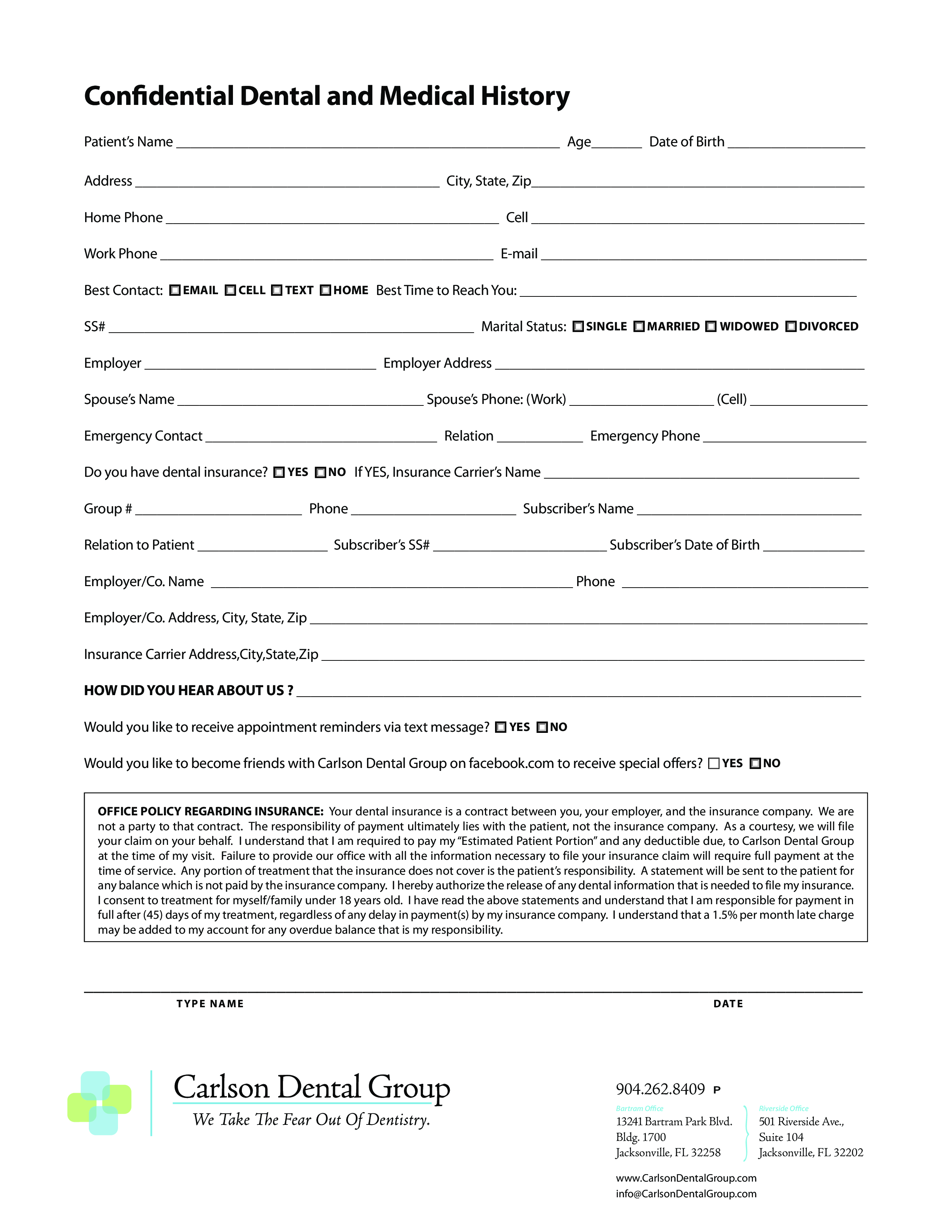
Dental Health History Form & Template Free PDF Download
Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. Both doctor and patient are encouraged to. Sample health history.
Family Health History Form Template Master Template
This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical conditions they might have,. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Sample health history forms are available through the.
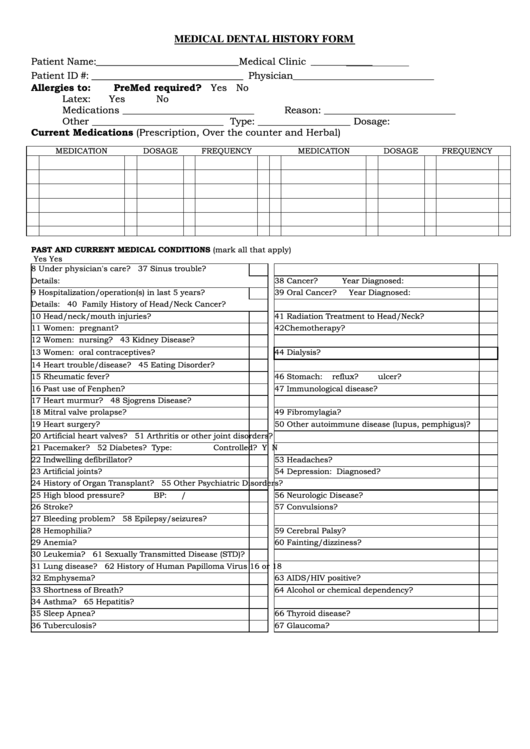
Medical Dental History Form printable pdf download
Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. This form provides a detailed overview of a patient's medical.
Printable Dental Medical History Form Template Printable Templates
Medical information please mark (x) your response to indicate if you have or have not had any of the following diseases or problems. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. Both doctor and patient are encouraged to. Use the 2021 edition of the ada.
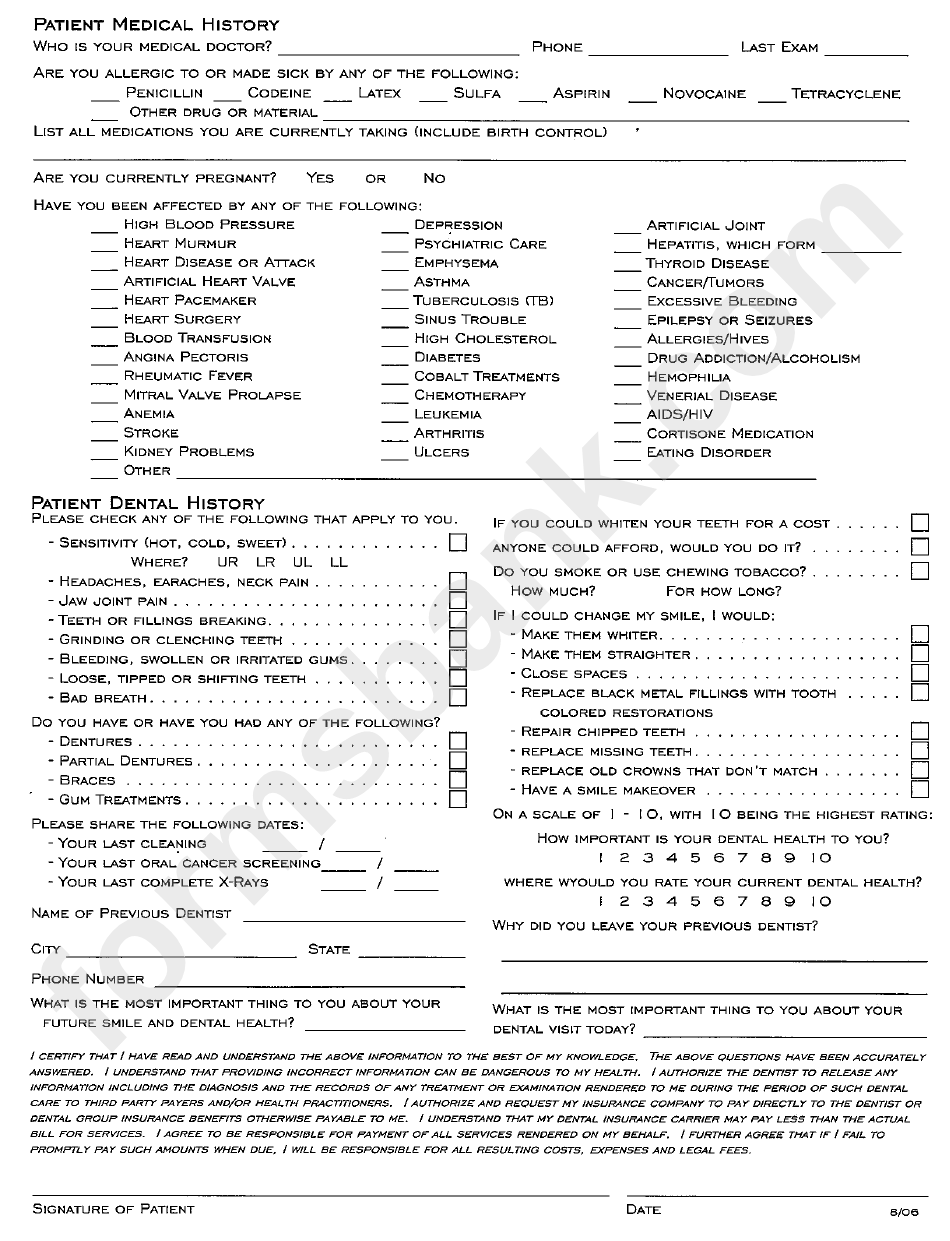
Patient Medical Dental History printable pdf download
This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical conditions they might have,. Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. Sample health history forms are available through the.
Printable Medical History Form For Dental Office Printable Word Searches
Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Both doctor and patient are encouraged.
This Form Provides A Detailed Overview Of A Patient's Medical History, Including A Patient's Dental History, Previous Dental Treatments, Specific Medical Conditions They Might Have,.
Both doctor and patient are encouraged to. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online.